Naloxone Dosing Calculator
How to Use This Calculator
This tool follows the 4-2-1 dosing protocol for opioid overdose reversal. Enter the opioid type and current respiratory rate (if known), then calculate.
Recommended Protocol
Critical Safety Notes
- Multiple naloxone doses may be needed for synthetic opioids like fentanyl
- Re-narcotization is common - require 4+ hour monitoring after reversal
- Naloxone may trigger severe withdrawal symptoms
- Capnography detects respiratory depression 62 seconds earlier than pulse oximetry
When someone takes an opioid - whether it's prescription painkillers, heroin, or illicit fentanyl - their breathing can slow down so much that it stops. This isn't a rare side effect. It's the main reason people die from opioid overdoses. In 2022 alone, over 107,000 people in the U.S. died from drug overdoses, and 80% of those involved opioids. Most of those deaths happened because opioids shut down the brain's ability to control breathing. This isn't just about feeling sleepy. It's about your body literally forgetting how to breathe.
How Opioids Kill: The Brain’s Breathing Switches
Opioids don’t just make you drowsy. They target specific clusters of neurons in the brainstem that control breathing. For decades, doctors thought the problem was simple: opioids made the whole respiratory system sluggish. But new research shows it’s far more precise - and dangerous.
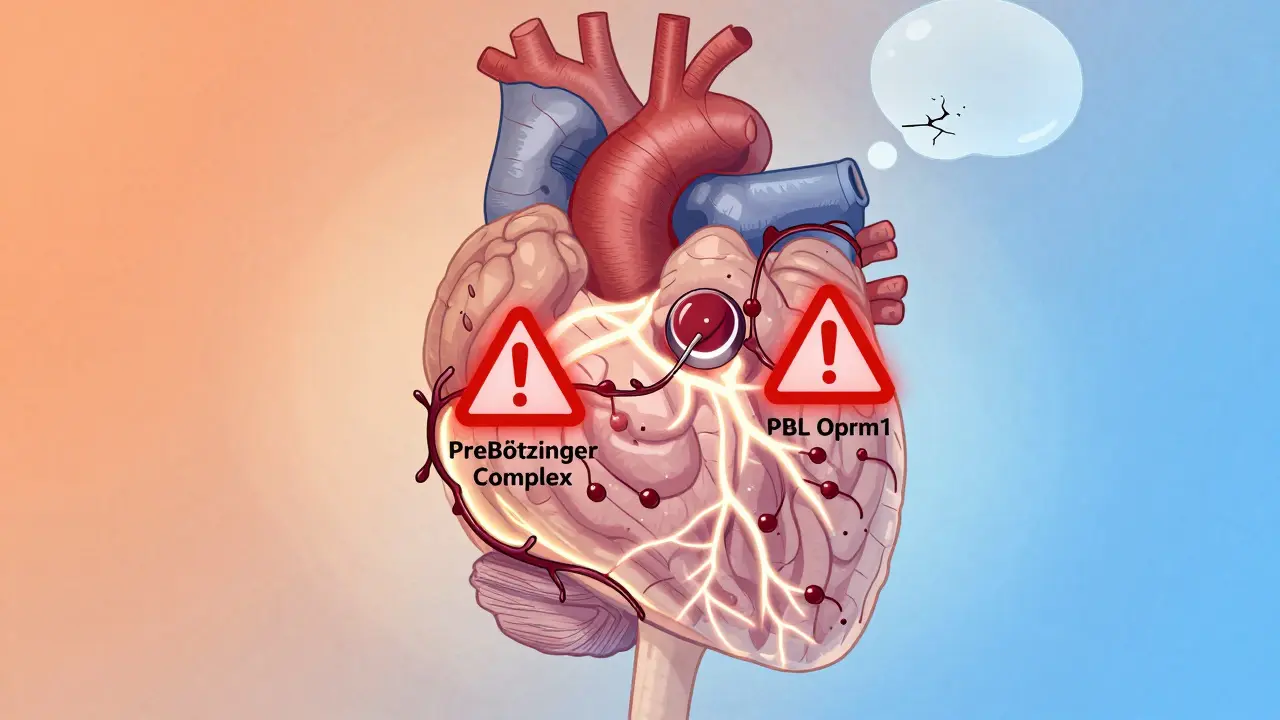
One key group of neurons, called PBL Oprm1 neurons in the lateral parabrachial nucleus, acts like a master switch for breathing rhythm. When opioids bind to these cells, they hyperpolarize them - essentially flipping a biological off-switch. A 2021 study in PNAS found that when these neurons are chemically silenced, breathing drops by over 50%, even without any drugs. When opioids are given, they lock these neurons in that off state. The result? Breathing becomes shallow, slow, and eventually stops.
Another critical area is the preBötzinger Complex, the brain’s natural pacemaker for breathing. Here, opioids do two things at once: they make individual neurons less likely to fire (reducing spike count by over 60%), and they break the connections between those neurons, so even if some are still active, they can’t coordinate. This dual attack explains why breathing doesn’t just slow - it collapses.
Why Expiration Gets Stuck
Most people think of breathing as inhaling and exhaling equally. But in opioid-induced respiratory depression, the problem isn’t with taking a breath - it’s with letting it out.
Studies using animal models show that opioids dramatically prolong the expiratory phase. In rats, expiratory time jumped from 0.82 seconds to over 2.3 seconds after a single dose of morphine. That’s not a small delay - it’s enough to prevent the next breath from starting. The brain’s rhythm gets stuck in the “out” phase, and the next inhale never happens. This is why respiratory rate drops so sharply while tidal volume (the amount of air moved per breath) stays relatively unchanged. The lungs aren’t emptying poorly - they’re not filling at all.
Why Naloxone Often Fails
Naloxone (Narcan) is the go-to drug to reverse overdoses. It works by kicking opioids off the receptors. But here’s the catch: it doesn’t fix everything.
Because opioids disrupt both the firing of neurons AND the communication between them, naloxone has to overcome two separate problems. Dr. Jan-Marino Ramirez explains it this way: “We need to reverse both the cellular silence and the broken wiring.” That’s why many patients need multiple doses of naloxone - and why some still die even after being revived.
Real-world data confirms this. A 2023 survey of 1,247 anesthesiologists found that nearly 70% had seen patients who didn’t fully recover breathing after standard naloxone doses. At Bellevue Hospital in New York, 41% of patients reversed with naloxone needed a second dose within 90 minutes because the opioid’s effects outlasted the reversal. This is especially true with fentanyl and carfentanil - synthetic opioids that bind much tighter and last longer than morphine or heroin.

What Happens When Breathing Stops
Without oxygen, your brain starts to shut down. Arterial oxygen saturation - the measure of how much oxygen is in your blood - drops below 90% in just 5 to 7 minutes after breathing stops. At that point, brain cells begin to die. Permanent injury, coma, or death can follow within minutes. This isn’t a slow process. It’s a race against time.
That’s why early detection is everything. Pulse oximeters - the devices that clip on your finger - are too slow. They only show low oxygen after breathing has already failed. But capnography - which measures carbon dioxide levels in exhaled air - catches trouble 62 seconds earlier on average. It shows rising CO2 levels as breathing slows, even before oxygen drops. In a 2022 Johns Hopkins study, 89% of critical care nurses called capnography “essential” for spotting OIRD before it’s too late.
What Clinicians See in Real Life
Emergency room staff and paramedics are on the front lines. One paramedic on Reddit, u/EmergencyMedic87, wrote: “Fentanyl overdoses just don’t bounce back like heroin did. You need continuous monitoring for 4+ hours.”
That’s because opioids like fentanyl have a long half-life. Even after naloxone brings someone back, the drug is still in their system. As naloxone wears off (in 30-90 minutes), the opioid can re-bind to receptors, and breathing shuts down again. This is called “re-narcotization.” It’s why hospitals now require patients to be monitored for at least 4 hours after reversal.
There’s another hidden problem: withdrawal. Naloxone doesn’t just reverse overdose - it triggers full opioid withdrawal. Many patients panic, become violent, or leave the hospital against medical advice. Dr. Sarah Wakeman at Mass General documented that 22% of patients refused further care after naloxone because they couldn’t handle the sudden pain and anxiety.
The New Tools: Monitoring and Next-Gen Reversals
By 2024, the FDA approved the first device specifically designed to predict OIRD before it happens: the RespiRhythm Monitor. It doesn’t measure breaths or oxygen. Instead, it detects subtle changes in skin impedance caused by activity in the parabrachial nucleus. In trials, it predicted respiratory depression 83 seconds before breathing slowed - giving clinicians a critical window to act.
On the drug side, new compounds are emerging. One called Brix51 targets GPR83 receptors in the same brain region that opioids hijack. In Phase II trials, it restored 78% of normal breathing without affecting pain relief. Another, TAK-861, is a “biased agonist” - it activates opioid receptors for pain relief but avoids the ones that shut down breathing. In primate studies, it delivered 94% of the pain relief of morphine with only 12.7% of the respiratory depression.
What You Need to Know
- Respiratory depression from opioids is not about sedation - it’s a neurological shutdown.
- Expiratory pause longer than 1.5 seconds is a red flag - even if breathing rate looks okay.
- Capnography detects OIRD earlier than pulse oximetry - use it whenever possible.
- Naloxone is lifesaving, but it’s not a cure. Reversal often requires multiple doses and long-term monitoring.
- Fentanyl and carfentanil require higher naloxone doses - standard kits may not be enough.
- Patients who are reversed must be observed for at least 4 hours to prevent re-narcotization.
Why This Matters
Over 80% of opioid deaths are preventable - if we understand the real mechanism. It’s not just about reducing drug use. It’s about recognizing the exact moment breathing begins to fail. It’s about using the right tools - capnography, longer monitoring, better reversal agents - before it’s too late.
The science has changed. The treatments are evolving. But the clock still ticks - and every second counts when someone stops breathing.
Can opioids kill you even if you take them as prescribed?
Yes. Even when taken exactly as directed, opioids can cause respiratory depression, especially in people who are opioid-naive, elderly, or have lung conditions like sleep apnea. The risk increases with higher doses, long-acting formulations, or when combined with alcohol, benzodiazepines, or other sedatives. Monitoring and low starting doses are critical for safety.
Why does naloxone sometimes not work?
Naloxone may not fully reverse respiratory depression if the opioid is a potent synthetic like fentanyl or carfentanil, which bind much tighter to receptors. It also doesn’t fix the broken neural communication in the brainstem - only kicks the opioid off. Multiple doses are often needed, and the effect of naloxone wears off faster than the opioid, leading to re-narcotization.
Is capnography really better than pulse oximetry for detecting opioid overdose?
Yes. Capnography detects rising CO2 levels as breathing slows - often 60 seconds before oxygen drops. Pulse oximetry only shows low oxygen after breathing has already failed. For opioid-induced respiratory depression, where the issue is reduced breathing rate (not poor oxygen exchange), capnography is the gold standard for early warning.
What’s the 4-2-1 rule for naloxone?
The 4-2-1 rule is a titration protocol: give 0.4 mg IV every 2 minutes until the respiratory rate exceeds 12 breaths per minute. This approach reduces the risk of precipitating severe withdrawal while ensuring enough naloxone is given to reverse respiratory depression. Studies show it has an 87% success rate in restoring breathing without causing extreme agitation.
Can you overdose on opioids without using them intravenously?
Absolutely. Opioid overdose can happen with oral pills, patches, or illicit powders snorted or smoked. The route of administration affects how fast the drug hits the brain - smoking or injecting fentanyl causes rapid collapse in under 5 minutes - but even slow-release pills can build up to dangerous levels over time, especially in people with reduced liver function or who are taking other medications.
Why are fentanyl analogs so dangerous?
Fentanyl is 50-100 times more potent than morphine. Carfentanil, used for elephant sedation, is 10,000 times stronger. A few micrograms can stop breathing. Standard naloxone auto-injectors (2 mg) often can’t reverse these - multiple doses are needed. Many street drugs are laced with fentanyl without the user’s knowledge, making accidental overdose extremely common.
What Comes Next
The tools are getting better - smarter monitors, smarter drugs. But until these become standard everywhere, the biggest risk remains the same: people don’t know what to look for. Breathing isn’t just slow - it’s absent. And by the time your fingers turn blue, it’s already too late. Recognizing the early signs - long pauses between breaths, shallow breaths, unresponsiveness - could save a life. And sometimes, that’s all it takes.
gemeika hernandez
March 18, 2026 AT 17:27Nicole Blain
March 19, 2026 AT 13:23Kathy Underhill
March 20, 2026 AT 02:13Ryan Voeltner
March 22, 2026 AT 02:00Emily Hager
March 23, 2026 AT 19:50Jeremy Van Veelen
March 24, 2026 AT 13:53jerome Reverdy
March 26, 2026 AT 10:16Andrew Mamone
March 28, 2026 AT 01:01MALYN RICABLANCA
March 28, 2026 AT 05:17gemeika hernandez
March 29, 2026 AT 06:26